![]()

CORONAVIRUSES AND COVID-19APPENDIX A
Why use a mask in a pandemic?
Dr Richard Hunt
Professor
Department of Pathology, Microbiology and Immunology
University of South Carolina School of Medicine
What should happen after lockdown restrictions are eased?
Why you should wear a mask
|
|
Population |
Cases |
Deaths* |
Stay home order |
Mask Use |
|
|
New York City |
8.3 million |
202,000 |
21,000 (2,530) |
20th March |
Little |
|
|
London |
8.9 million |
27,000 |
5,000 (561) |
23rd March |
Little (<20%) |
|
|
Tokyo |
14 million |
5,221 |
302 (22) |
None |
97% |
|
|
Hong Kong |
7.5 million |
1,066 |
4 (0.5) |
None |
99% |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sweden |
10.3 million |
37,000 |
4,395 (427) |
None |
2% |
|
|
UK |
67.9 million |
275,000 |
39,000 (574) |
23rd March |
13% |
|
|
Vietnam |
95.5 million |
328 |
0 |
None |
86% |
|
|
Figures as of third week of May,
2020 Mask use and populations: Wikipedia Other numbers: Johns
Hopkins University |
||||||
Correlation is not necessarily an indication of causation
At the beginning of the pandemic, many countries tried to stem the spread of Covid-19 by restricting interactions between people including requiring people to “shelter-in-place” and/or asking them to stay at least two meters apart, that is social distancing. In many cases this has been successful in reducing the reproduction factor, Rt, the number of people infected by one infected person. This mitigation of the spread of the disease was designed to reduce the peak of infections so that hospital facilities would not be overwhelmed. In some cases, such measures have done more than flatten the curve, they have reduced the Rt below 1 so that one infectious person infects less than one uninfected person. When this happens, the disease is likely to peter out. Clearly, the ideal would be an Rt of zero (i.e. no new infections). While these measures have lowered the number of infections and daily deaths, the virus has not gone away and there remain many infected people in the population. In many countries, the number of new daily cases is still rising (late May 2020) and if it does prove possible to eradicate the virus in one region or country, there is always the strong possibility that infections will be reintroduced from outside.
In the United States, many states started easing lockdown restrictions in mid-May, 2020, even while some states such as Texas and Alabama were recording increasing numbers of new cases each day. In the US as a whole, by late May, there had been 1.6 million confirmed cases of Covid-19 which, because of lack of testing, is probably a gross underestimate as many cases, especially in younger people, go undetected. For example, in South Carolina it is estimated that around 86% of infections have not been detected because of lack of testing. However, if there were really only 1.6 million cases in the US, this would mean that only 0.5% of the population had been infected. In Germany, and South Korea, where testing has been much more effective, the proportions of the population thought to be infected are 0.2 and 0.02% respectively. Thus, whatever the true number of infected people, it is only a very small proportion of the population and most of us are naïve with respect to the disease as there was no pre-exiting immunity to the SARS CoV-2 virus.
Lockdowns cannot go on forever as they cause too much economic damage. By the end of May, 2020, US unemployment had reached 20% and in the US, where health insurance is often tied to employment, up to 27 million people may have lost their health insurance at the very time that it was most needed. As a result, the loss of health insurance will make fewer people seek medical care just when it is required.
Inevitably when people interact more as “stay-in-place” restrictions are lifted, the Rt will rise and the pandemic is likely to break out again. So what should we do?
There is no vaccine against SARS CoV-2 and although many laboratories are racing to make one, the likelihood that it would be available before mid-2021 is very optimistic indeed. Forty years ago, at the height of the AIDS epidemic, many attempts at a vaccine were made and a vaccine was said to be “just around the corner” but forty years later the corner has not been turned and there is no anti-HIV vaccine. However, the discovery of HAART (Highly Active Anti-Retroviral Therapy) has made AIDS a tractable disease and recently there has been less interest in anti-HIV vaccines.
As far as Covid-19 is concerned, there are no effective (May 2020) pharmaceutical interventions; in the clinic, the highly touted hydroxychloroquine has shown little efficacy at best and dangerous side effects because of alterations in heart functions at worst.
Thus, in the absence of pharmaceutical interventions, we are left with non-pharmaceutical interventions. If “staying-in-place” is no longer an option, social distancing and barrier methods between infected and uninfected people are of the utmost importance and this brings us to masks.
There has been some confusion about the usefulness of masks. The World Health Organization originally recommended against them as they might give a false sense of security. But now it and the Centers for Disease Control and Prevention are recommending them as the evidence that they are effective becomes clearer. The CDC recommend all people wear cloth face masks when in public, reserving surgical masks and N95 masks for healthcare workers.
There are two ways that face masks work:
They stop an infected person breathing or sneezing out the virus as aerosolized droplets.
They stop an uninfected person being exposed to the virus when close to an infected person.
Any type of general mask is likely to decrease viral exposure and infection risk on a population level, in spite of imperfect fit and even home-made masks may confer a significant degree of protection (van der Sande et al., 2008).
Masking is particularly important in a disease like Covid-19 in which people are infectious for five to six days before they exhibit symptoms or even know that they have the disease. Indeed, many infected people never exhibit symptoms at all but they are still capable of spreading the virus. In Singapore, it has been estimated that the proportion of pre-symptomatic transmission was 48% and in Tianjin, China, 62% (Ganyani, T et al., 2020.).
So let’s look at some of the evidence that near universal use of masks could be a major step in the Covid-19 pandemic as economies open up. If no steps are taken to lessen infection (i.e. lower the Rt), we have just put off the pandemic for a later time. Could mask use reduce the Rt below 1 so that the disease just peters out?
 Figure 1
Figure 1A sneeze in progress, revealing the plume of salivary droplets that are expelled in a large cone-shaped array from the open mouth. This demonstrates why covering the mouth when coughing or sneezing is important to protect others from germ exposure. CDC: Public domain.
CAN NON-SURGICAL MASKS FILTER OUT VIRUSES?
Viruses were first discovered as non-filterable agents of disease and are small, in the case of a Corona virus around 100nm; but we need to remember that we are not coughing up millions of virus particles alone.
Respiratory viruses are normally expelled as an aerosol, that is in drops of liquid (figure 1) that may be 10 micrometers (µm) or more in diameter. So can home-made masks filter out droplets of the size that are in a typical sneeze? This depends on the pore size of the mask material and, thus, the nature of the cloth used to make the mask. Here are some results of a study of materials that might be commonly used in mask manufacture (Konda et al., 2020).
|
Filter efficiency (%) |
||
|
Sample/fabric |
Droplet
size: |
Droplet
size: |
|
N95 mask (with no gap) |
85 ± 15 |
99.9 ± 0.1 |
|
N95 (with gap) |
34 ± 15 |
12 ± 3 |
|
surgical mask (no gap) |
76 ± 22 |
99.6 ± 0.1 |
|
surgical mask (with gap) |
50 ± 7 |
44 ± 3 |
|
cotton quilt |
96 ± 2 |
96.1 ± 0.3 |
|
quilter’s cotton (80 TPI+), 1 layer |
9 ± 13 |
14 ± 1 |
|
quilter’s cotton (80 TPI+), 2 layers |
38 ± 11 |
49 ± 3 |
|
flannel |
57 ± 8 |
44 ± 2 |
|
cotton cloth (600 TPI+), 1 layer |
79 ± 23 |
98.4 ± 0.2 |
|
cotton cloth (600 TPI+), 2 layers |
82 ± 19 |
99.5 ± 0.1 |
|
Chiffon (90% polyester and 10% Spandex), 1 layer |
67 ± 16 |
73 ± 2 |
|
chiffon, 2 layers |
83 ± 9 |
90 ± 1 |
|
natural silk, 1 layer |
54 ± 8 |
56 ± 2 |
|
natural silk, 2 layers |
65 ± 10 |
65 ± 2 |
|
natural silk, 4 layers |
86 ± 5 |
88 ± 1 |
* In a sneeze, most of the droplets are probably much
bigger than 300nm.
+ Threads per inch
Thus, it would appear that masks made of cotton, natural silk, and chiffon can provide good protection, typically above 50% in the entire 10 nm to 6,000 nm range, provided they have a tight weave (high thread count).
Other data using hamsters also suggest that use of masks may be very important in pandemic control. Dr Yuen Kwok-yung at the University of Hong Kong and his colleagues have shown (South China Morning Post, May 17) that surgical masks protect hamsters when they are placed between two cages with air flow travelling from infected to healthy animals. They found non-contact transmission of the virus was reduced by more than 60 percent by the masks. Two thirds of the healthy animals were infected within a week if no masks were used whereas the infection rate fell to just over 15 percent when surgical masks were put on the cage of infected animals and by around 35 percent when placed on the cage with the healthy hamsters. Importantly, hamsters that become infected when masks were used had less virus (i.e. lower viremia) than those infected without a mask. This is important because the lower the viremia, the better chance the immune system has to neutralize the virus.
This would suggest that masks are likely to be useful in reducing transmission of Covid-19 but how useful? Could transmission be lowered enough to reduce the Rt below 1?
A group of pandemic modelers from universities in Cambridge, Berkeley, Hong Kong, Helsinki and Paris (Kai et al., 2020) have shown that masks could be very useful, especially as lockdowns are eased and may help reduce the Rt to below 1 and hence diminish the pandemic, especially if they are used by the majority of the population. They found that there was a significant impact under near universal masking, that is when at least 80% of a population is wearing masks, versus much less impact when only 50% or less of the population is wearing masks. In addition, there was significant impact when universal masking is adopted early rather than late in an outbreak.
To validate their theoretical models, they compared their predictions with whether regions have universal masking cultures or policies. Their results showed a close correlation between early universal masking and successful suppression of daily case growth rates and/or reduction from peak daily case growth rates, as predicted by the theoretical simulations.
Let’s look at this is more detail since universal masking may be imperative as a non-pharmaceutical intervention in fighting the Covid-19 pandemic although, so far, as countries emerge from a lockdown, there seems little being done to enforce this. Kai et al. make several recommendations:
1. Masking should be mandatory or strongly recommended for the general public when in public transport and public spaces, for the duration of the pandemic.
2. Masking should be mandatory for individuals in essential occupations (such as health care workers, social and family workers, the police and the military, the service sector, construction workers, etc.) and medical masks and gloves or equally safe protection should be provided to them by employers. Cloth masks should be used if medical masks are unavailable.
3. Countries should aim to secure mass production and availability of appropriate medical masks for the entire population during the pandemic.
4. Until supplies are sufficient, members of the general public should wear non-medical fabric face masks when going out in public with medical masks being reserved for essential workers.
5. The authorities should issue masking guidelines to residents and companies regarding the correct and optimal ways to make, wear and disinfect masks.
6. The introduction of mandatory masking will benefit from being rolled out together with campaigns, citizen initiatives, the media, NGOs, and influencers in order to avoid a public backlash in societies not culturally accustomed to masking. Public awareness is needed that “masking protects your community, not just you”.
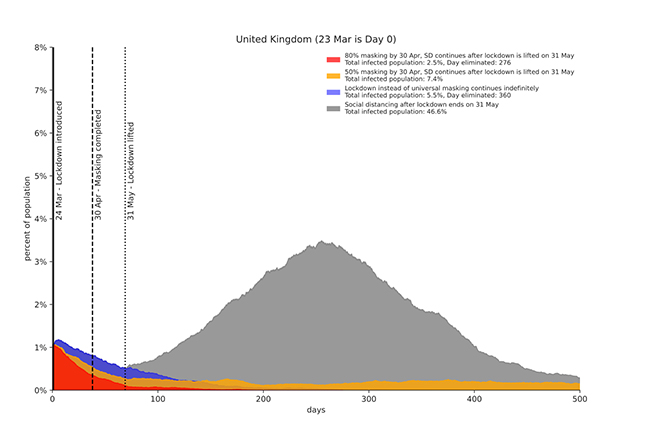 Figure 2
Figure 2Simulation results for a representative scenario: universal masking at 80% adoption (red) flattens the curve significantly more than maintaining a strict lockdown (blue). Masking at only 50% adoption (orange) is not sufficient to prevent continued spread. Unchecked spread of the disease, however, occurs after replacing the strict lockdown with social distancing on May 31 without masking.
From: Kai et al., 2020
What is the evidence to support this?
The authors assume that the rate of transmission would be reduced by 50% using a mask, which they say is a conservative estimate and would agree with the above data on various mask materials. Using their model, they look at four scenarios for the United Kingdom where a lockdown was instituted on March 23, 2020.
Social distancing with 80% masking by April 30 with social distancing continuing after lockdown is lifted on May 31 (red in figure 2).
Social distancing with 50% masking by April 30 with social distancing continuing after lockdown is lifted on May 31 (yellow in figure 2).
Lockdown continues indefinitely without masking (blue in figure 2).
Only social distancing after the lifting of lockdown on May 31 (gray in figure 2).
They found that universal masking with 80% adoption (scenario 1 - red) is actually better than continuing a strict lockdown (scenario 3 - blue). However, masking at only 50% adoption (scenario 2 - orange) is not enough to prevent continued spread. Lifting the strict lockdown but with continued social distancing on May 31 without masking results in unchecked spread (scenario 4 - grey). Without masking, but with continued social distancing after the lockdown is lifted, the infection rate soars and almost half of the population becomes infected.
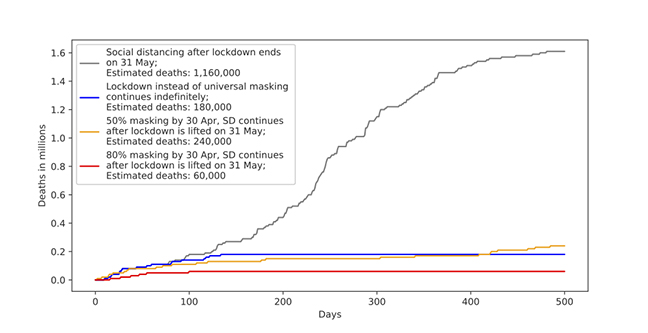 Figure 3.
Figure 3.Simulation results for a representative scenario: universal masking at 80% adoption (red) results in 60,000 deaths, compared to maintaining a strict lockdown (blue) which results in 180,000 deaths. Masking at only a 50% adoption rate (orange) is not sufficient to prevent continued spread and eventually results in 240,000 deaths. Replacing the strict lockdown with social distancing on May 31 without masking results in unchecked spread.
From: Kai et al., 2020
A high degree of masking thus has a considerable effect on the spread of the disease:
With only social distancing after end of lockdown, 46% of the population would become infected and the disease just spreads until it finally peters out due to herd immunity.
With 50% masking with social distancing continuing after lifting lockdown, there is a considerable improvement with 7.4% of the population infected. But the disease continues to circulate spawning new infections and clusters of infections.
With lockdown continuing indefinitely, 5.5% of the population becomes infected but the disease should peter out after about a year.
With 80% masking with social distancing continuing after lifting lockdown, 2.5% of the population becomes infected and the disease is eliminated after about 9 months (276 days). This elimination supposes that the community is not reinfected from other regions that have not instituted near universal masking.
Masking also reduces the number of deaths. Figure 3 shows the results for each scenario:
Universal masking at 80% adoption (red) with continued social distancing results in 60,000 deaths in the UK.
Maintaining a strict lockdown (blue) results in 180,000 deaths.
Masking at only a 50% level (orange) with continued social distancing is not sufficient to prevent continued spread and eventually results in 240,000 deaths.
Replacing the strict lockdown with social distancing on May 31 without masking results in unchecked spread and over 1.1 million deaths after 500 days.
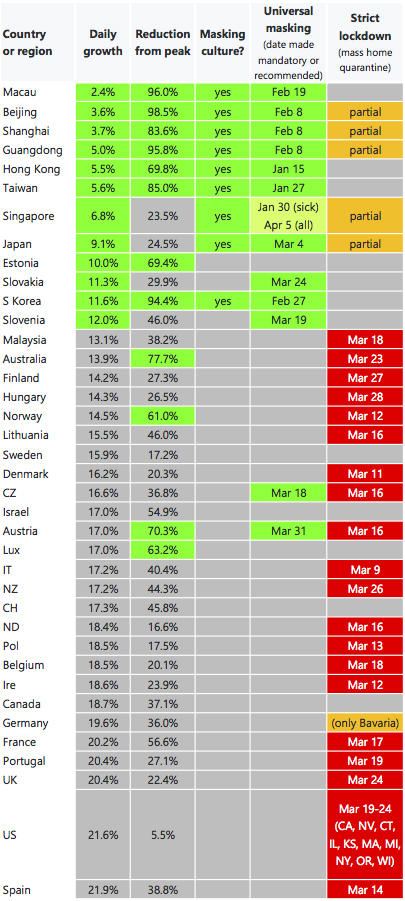 Figure 4.
Figure 4.Epidemic daily growth and reduction from peak daily growth, together with masking culture, universal masking policy, and lockdown policy, from January23 to April 10, 2020 for selected list of countries or provinces with high GDP PPP per capita in Asia, Europe and North America. Universal masking was employed in every region that handled COVID-19 well. Sources: John Hopkins, Wikipedia, VOA News, Quartz, Straits Times, South China Morning Post, ABCNews, Time.com, Channel New Asia, Moh.gov.sg, Reuters, Financial Times, Yna.co.kr, Nippon.com, Euronews, Spectator.sme.sk
From: Kai et al., 2020
Additional modeling showed that when the level of masking in the population is high and social distancing continues after the end of the lockdown, even a small barrier to individual infection transmission can multiply into a substantial effect at the level of communities and populations.
But these are just models and models are only as useful as the assumptions used to make them. It would seem that a 50% reduction of infection resulting from near universal masking is reasonable but the accuracy of the model is best judged by seeing what eventually pans out which may be too late. However, second best is to see how the model fits with what has already happened. Some countries have a masking culture in which a high proportion of the population already wears masks. These include China, Japan and countries of south-east Asia. In China, this habit may have arisen as a result of air pollution and previous health alarms such as SARS and avian flu. Indeed, retrospective case‐control studies showed that mask use in Hong Kong may have offered significant protection against SARS (Lau JTF, Tsui H, Lau M, Yang X. SARS transmission, risk factors and prevention in Hong Kong. Emerging Infectious Diseases, 2004; 10:587–592). Other countries (particularly in Europe) mandated universal masking early in the Covid-19 pandemic. Thus, we can ask: Has the growth of Covid-19 cases been reduced in regions where we already have a large amount of masking? Does the experience of these countries fit the epidemiologists’ model? The answer to both questions is yes.
Kai et al. looked at successful management of an epidemic as defined by:
Success in suppressing the daily growth of new cases from the start of the epidemic. Success was defined as being below 12.5% daily growth (that is with the number of cases doubling every 6 days or longer) once the number of detected cases first reached 30.
Success in reducing the number of new cases after a peak of infections. This was defined as a significant (>60%) reduction of new cases calculated as the average of the last five days before April 10, 2020 compared to the average of the three highest number of daily new cases up to April 10, 2020 starting from the date when the number of detected cases first reached 30.
They found that an overwhelming majority of countries or regions that best managed Covid-19 outbreaks up to April 10, 2020 as judged by successful suppression of daily growth and/or reduction from peak were countries or regions with either established universal masking cultures or mandatory orders or recommendations. As shown in figure 4, these countries or regions (shown in green) include Taiwan, South Korea, Singapore, Japan, Hong Kong, Macau, and Chinese provinces including Beijing, Shanghai, and Guangdong. Masking in public has been required in Taiwan, metropolitan areas in China, Japan, South Korea, and others. In contrast, countries (indicated in red) with strict lockdowns and mass testing, tracking and quarantining but no universal masking did not achieve the same level of Covid-19 control as of April 10, 2020. This close correlation between early universal masking and successful management of Covid-19 outbreaks bears out the modeling predictions. In Hong Kong, public masking adherence has been very high (97-98%). Other data confirm the need for universal masking to control the Covid-19 outbreaks although we should note that correlation and causation are not the same.
Masking should also be as early as possible for maximum protection of the population. Singapore initially encouraged people to wear masks but only when feeling unwell. Then the government changed its recommendations and distributed reusable masks. In contrast, the Hong Kong government advised all citizens to wear masks in crowded places and public transportation. Figure 4 shows that lower daily growth rate and reduction from peak were better for Hong Kong than Singapore.
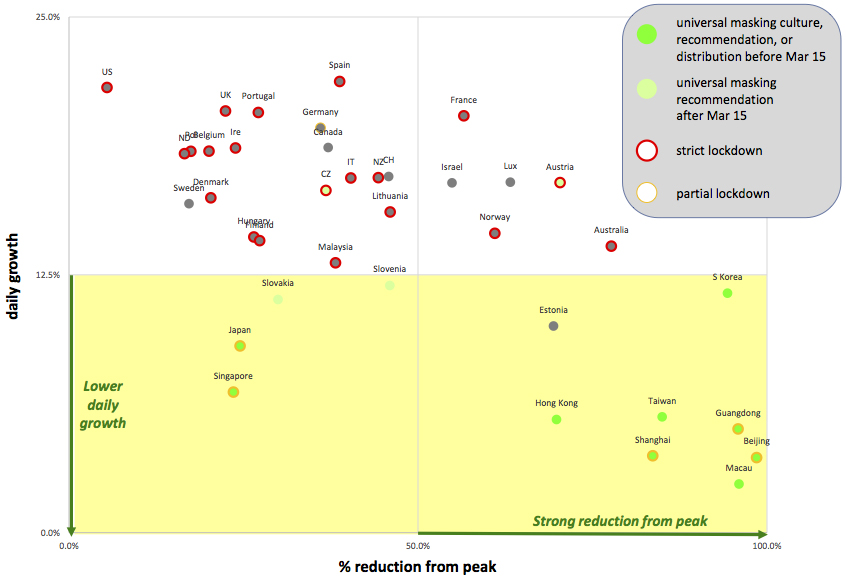 Figure 5.
Figure 5.Visual representation of epidemic daily growth versus percentage reduction from peak daily daily growth in quadrants showing the impact of universal masking on epidemic control: and reduction from peak, from January 23 to April 10, 2020 for selected list of countries or provinces with high GDP PPP per capita in Asia, Europe and North America. Masking is nearly perfectly correlated with lower daily growth or strong reduction from peak growth of COVID-19. From: Kai et al., 2020
In figure 5, the daily growth was plotted against percentage reduction from peak. Green points represent places with early universal masking and fall within the lower two quadrants representing successful management of the disease. Red points represent places with strict lockdowns but not universal masking. Most of these fall in the two upper quadrants representing less successful management of the disease. Again, the strong correlation of a high level of masking with successful control of case growth case growth supports the model’s predictions.
Masking has an additional benefit even when masks are not perfect. By filtering droplets exhaled by an infected person, the dose received by someone nearby should be much reduced if not totally eliminated. There is evidence that a lower dose of virus can lead to a milder infection (presumably because it can be overcome more rapidly by the immune system) and therefore a better outcome for the infected person.
Further evidence supports mask use and continued social distancing when lockdowns are lifted. Chu et al. reviewed 172 studies of the spread of SARS, MERS and Covid-19 (all caused by Coronaviruses) carried out in sixteen countries. All of these studies were observational with no randomized trials. They performed a meta-analysis of 44 comparative studies (that is those that included comparisons between people who social distanced and wore masks with those who did not) of 25,697 patients with the three Coronavirus diseases. As, expected, they found that viral transmission fell with greater social distancing, that is protection was greater the more people kept apart. One meter of physical distancing was associated with a large reduction in infection (an infection rate of about 3%, down from 13% when less than one meter apart). As might be predicted, two meters was more effective and they project that three meters distancing should result in little infection. The projected risk drops by about half for every meter of distancing up to 3 meters. The use of facemasks was also associated with a lower infection risk. N95 masks were better than cloth masks or surgical masks and eye protection also was associated with less infection. Face shields were most effective but even glasses may offer some protection . In studies that addressed eye protection there was an absolute risk of 5·5% with eye protection versus 16·0% with no eye protection.
In conclusion, it is apparent that suppression of daily growth and reduction from peak, two measures of success in infection control correlate very well with early and high levels of masking. Early mass masking is an alternative to continued lockdown which is becoming increasingly difficult to sustain economically.
In emerging from lockdowns, countries need to:
Test, track and quarantine
Continue social distancing
Provide adequate personal protective equipment and for the general population, this means the mandatory use of masks.
![]() Return to the Coronavirus page
Return to the Coronavirus page
![]() Return to the Virology section of Microbiology and Immunology On-line
Return to the Virology section of Microbiology and Immunology On-line
This page last changed on
Tuesday, June 02, 2020
Page maintained by
Richard Hunt