Brief review of influenza
virus structure and properties
Discussion of viral pathogenesis and disease,
genetics, epidemiology, prevention and treatment
INTRODUCTION
Every year in the United States, millions of people get the flu.
The intensity of the epidemic depends on several factors including:
The types of influenza virus that are circulating in the
population
The efficacy of the annual flu vaccine
The proportion of the population that is vaccinated
Many thousands, in a bad year many hundreds of thousands, of
patients are hospitalized and some die. In many cases, influenza-related
mortality is not reported or recorded and statistical models are used to
estimate the number of deaths. CDC estimates that from 1976 to 2007 in the
United States, the number of annual deaths from influenza ranged from a low of
around 3,000 to a high of around 49,000.
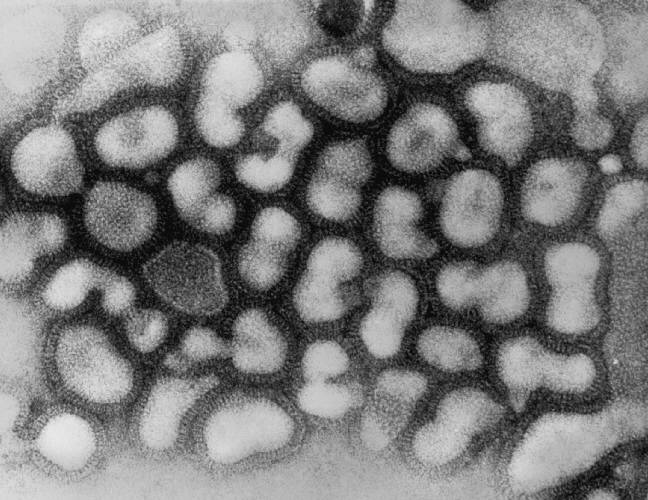
True influenza is an acute
infectious disease caused by a member of the orthomyxovirus family (figure 1): influenza
virus A (figure 2), B or, to a much lesser extent, influenza virus C (figure 3). However, the term 'flu'
is often used for any febrile respiratory illness with systemic symptoms that
may be caused be a myriad of bacterial or viral agents as well as influenza
viruses.
Influenza outbreaks
usually occur in the winter in temperate climates. In the United States, the
'flu season usually starts in October or November and is at its height from
December to March (figure 4 - 6).
Figure 4 Number of specimens received for influenza testing per month
South Carolina DHEC
Figure 5
Peak months for flu activity over the past 21 years CDC
Disease potential
Major outbreaks of influenza
are associated with influenza virus type A or B. Infection with type B influenza
is usually milder than type A. Type C virus is associated with minor symptoms.
Proteins
The internal antigens (M1 and
NP proteins - figure 1) are the type-specific proteins (type-specific antigens) used to determine
if a particular virus is A, B or C. The M1 proteins of all members of each
type show cross reactivity. The NP proteins of all members of each type also
show cross reactivity.
The external antigens (HA and
NA) show more variation and are the subtype and strain-specific antigens. These
are used to determine the particular strain of influenza A responsible for
an outbreak.
The virus is spread person to
person via small particle aerosols (less than 10μm diameter) that can get into
the respiratory tract. It can also be spread via
fomites
since it can survive for a short time on surfaces and can be
spread by this route if the virus is introduced into the nasal mucosa before it
loses infectivity. The incubation period is short, about 18 to 72 hours.
Virus concentration in nasal and tracheal secretions remains high for 24 to 48 hours
after symptoms start and may last longer in children. Titers are usually high
and
so there are enough infectious virions in a small droplet to start a new
infection.
Site of infection
Influenza virus infects the epithelial cells of the
respiratory tract. The cells die, in part due to the direct effects of the
virus on the cell, and also possibly due to the effects of interferon. Cell
death at later times may also result from the actions of cytotoxic T-cells.
As a result, the efficiency of ciliary clearance is reduced, leading to impaired
function of the mucus elevator; thus there is reduced clearance of
infectious agents from the respiratory tract. Gaps in the protective
epithelium provide other pathogens with access to other cells; however,
viremia is very rare.
Recovery
Interferon may play a role by decreasing virus production. Many of the
symptoms of uncomplicated influenza (muscle aches, fatigue, fever) are
associated with the efficient induction of interferon. The cell-mediated
immune response is important in viral clearance. The antibody response is
usually not significant until after virus has been cleared. Repair of the
respiratory epithelium begins rapidly, but may take some time to complete.
A humoral antibody response
is the main source of protection. IgG and IgA are important in protection
against reinfection. Antibody to the HA protein is most important since this can
neutralize the virus and prevent the virus initiating the infection.
Neutralization frequently involves blocking of the binding of the virus to host
cells and may work at other steps involved in the entry and uncoating of the
virus. Antibody to the NA protein has some
protective effect since it seems to slow the spread of the virus. IgG persists
longer than IgA and so plays a more important role in long term immunity.
Clinical findings
The disease is usually most
severe in very young children (under 5 years of age) and the elderly. Young children
often lack antibodies to the influenza virus because of no prior exposure. In
addition, the small diameter of
components of the respiratory tract in the very young also means that inflammation and swelling can
lead to blockage of parts of respiratory tract, sinus system or Eustachian
tubes. Although children with risk factors for influenza complications have a
higher case fatality rate, the majority of pediatric deaths occur among children
with no high-risk conditions. In the elderly, influenza is often severe because
of an underlying decreased effectiveness of
the immune system and/or chronic obstructive pulmonary disease or chronic
cardiac disease.
CDC surveys show that each year about 114,000 people in the
United States
are hospitalized and many thousands may die because of the flu. Flu and
pneumonia together constitute the sixth leading cause of deaths in the United
States. Most flu fatalities
are 65 years and older. Children younger than 2 years old are as likely as those
over 65 to have to be hospitalized because of the flu. The 1918 Spanish flu
outbreak killed more than 500,000 people in the United States and more than 20
million worldwide. The 1968-69 "Hong Kong flu" outbreak led to more than 34,000
deaths in the United States.
H1N1 strain, the 2009 "swine flu", also gives rise to
gastro-intestinal symptoms (e.g. vomiting, diarrhea)
2. Pulmonary complications,
sequelae:
Croup
(acute laryngotracheobronchitis) in young children - symptoms include cough
(like a barking seal), difficulty breathing, stridor (crowing sound during
inspiration)
Primary influenza virus pneumonia
Secondary bacterial infection: This often involves
Streptococcus pneumoniae, Staphylococcus aureus, Hemophilus influenzae
The build up of fluids and lack of mucociliary clearance in the respiratory
tract provide a good environment for bacterial growth.
Complications often occur in patients with underlying chronic obstructive
pulmonary or heart disease. The underlying problems may not have been recognized
prior to the influenza infection.
3. Non-pulmonary
complications of influenza:
Myositis
- This is rare and more likely to be seen in children after influenza type B infection
Cardiac complications
Encephalopathy - Increased surveillance of hospital
patients less than 21 years of age in the state of Michigan in the United States
during the 2002 - 2003 flu season revealed eight cases of influenza-associated
encephalopathy (figure 6A). Two of these patients (aged two and five years) died. Similar
complications of influenza have been reported from Japan. Even when not fatal,
encephalopathy can have serious sequelae and this emphasizes the importance of
vaccination. Neither of the Michigan fatalities had been vaccinated.
Reye's
syndrome - The effects of influenza virus infection on the liver and brain are
particularly serious. In the liver fatty deposits are seen while in the brain
edema occurs. Reye's syndrome includes vomiting, lethargy and may result in
coma. It is rare, but approximately 40% of cases are fatal. The origin of
Reye's syndrome is unclear but seems to follow certain viral infections such
as influenza or chicken pox (varicella zoster/herpes zoster), especially if
they are in the young and especially if they have been treated with aspirin.
Aspirin is contraindicated for childhood or adolescent fevers because it is a
risk factor in the development Reye's syndrome. Acetaminophen and Ibuprofen
are apparently
not associated with Reye's syndrome.
Guillain-Barré
syndrome (acute idiopathic polyneuritis) - The cause of this syndrome
in the central nervous system is mysterious. It is an autoimmune disease
that can follow a viral or bacterial (e.g. Campylobacter jejuni) infection. Recent anti-influenza vaccines do not seem to increase the risk of developing
Guillain-Barre Syndrome.
The major causes of
influenza-associated death are bacterial pneumonia and cardiac failure. Ninety
per cent of deaths are in people over 65 years of age.
DIAGNOSIS
Firm diagnosis is by means of
virus isolation and serology. The virus can be isolated from the nose or a
throat swab. This is used to infect cells in culture (or eggs).
Hemadsorption
may be used to detect infected cells. Polymerase chain reaction (PCR) test are
being developed to detect viral RNA. Recently, rapid tests that can be used in a
physician's office have been approved.
Provisional diagnosis is often made clinically, based on knowledge of a current
outbreak of influenza combined with appropriate clinical symptoms (fever, cough,
runny nose, malaise).
EPIDEMIOLOGY
HA (hemagglutinin) protein
The HA protein is
involved in attachment and membrane fusion in the endosome of the infected cell.
The receptor binding site on the virus is in a pocket (figure 7) that is not exposed to the
immune system.
The antigenic domains are on the surface. These can be altered and the virus can
thus avoid a humoral response without affecting its ability to bind to the
receptor.
NA (neuraminidase) protein
The neuraminidase protein digests
sialic acid (neuraminic acid) - which most cells have on their surface. Since sialic acid is part of the virus receptor,
when the virus binds to the cell, it will be internalized (endocytosed). By late
in infection, the sialic acid will have been removed from the infected cell
surface by the neuraminidase making it is easier for the progeny virions to
diffuse away once they exit the cell. Neuraminidase is also involved in
penetration of the mucus layer in the respiratory tract.
Antigenic drift
Antigenic drift is due to mutation. Antibodies to the HA protein are
the most important in protection, although those to NA also play a role. Both
proteins undergo antigenic drift (i.e. accumulate mutations) and accumulate changes
such that an individual immune to the
original strain is not immune to the drifted one. Antigenic drift results in
sporadic outbreaks and limited epidemics.
Antigenic shift
Antigenic shift is due to reassortment.
In the case of influenza A, antigenic shift periodically occurs.
Apparently "new" HA and/or NA are found in the circulating viral
strains. There is little immunity (particularly if both proteins change, or if
new HA is present) and an epidemic/pandemic is seen.
Figure 6A
Number and percentage of signs and symptoms and conditions among influenza
patients in Michigan
Figure 7
The HA protein has a pocket that binds to the cell
receptor. Antibodies cannot get into the pocket. Since antigenic domains
are on the surface of the HA, these can be altered without altering
receptor binding. Cell enzymes cleave the receptor outside the cell but
the HA is only activated in an endosome
Figure 8
Types of influenza that predominated from 1995/6 to 1998/99
CDC
PANDEMICS CAUSED BY INFLUENZA A
Major antigenic shifts associated with influenza A
pandemics
Year
Sub type
Prototype strain
1947
H1N1
A/FM1/47
1957 (Asian flu)
H2N2
A/Singapore/57
1968 (Hong Kong flu)
H3N2
A/Hong Kong/68
1977
H1N1
A/USSR/77
1987
H3N2
No pandemic
Various strains circulated worldwide
Adapted from Ryan et al. Sherris Medical
Microbiology
Figure 9
Pneumonia and Influenza Mortality Surveillance for
122 US cities 2003-2006
Figure 10A
2001-2001 weekly US summary
Figure 10B
Avian influenza A (H5N1) virion, a type of bird flu virus which is a subtype
of avian influenza A. At this magnification, one may note the stippled
appearance of the roughened surface of the proteinaceous coat encasing the
virion. CDC
Figure 10 C
H7N9 Avian Flu. Negative stain electron micrograph.
CDC/ Cynthia S. Goldsmith and Thomas Rowe
Figure 10C
Genetic Evolution of H7N9 flu in China in 2013.
The eight genes of the H7N9 virus are closely related to avian influenza
viruses found in domestic ducks, wild birds and domestic poultry in Asia.
The virus likely emerged from “reassortment,” a process in which two or more
influenza viruses co-infect a single host and exchange genes. This can
result in the creation of a new influenza virus. Experts think multiple
reassortment events led to the creation of the H7N9 virus. These events may
have occurred in habitats shared by wild and domestic birds and/or in live
bird/poultry markets, where different species of birds are bought and sold
for food. As the above diagram shows, the H7N9 virus likely obtained its HA
(hemagglutinin) gene from domestic ducks, its NA (neuraminidase) gene from
wild birds, and its six remaining genes from multiple related H9N2 influenza
viruses in domestic poultry.
CDC
Where does a "new" HA and/or NA
come from? All sixteen HA and nine NA types circulate in ducks, some also circulate in
other animals. It appears that some animal, somewhere (possibly a pig), becomes
infected with both human and animal viruses, and that one of the reassortants contains genes for human internal
components but a new HA and/or NA segment from the animal virus. If this virus
reassortant can infect humans, it
will have mainly the same internal components as the current human virus, but new
envelope components resulting in little immunity in the population. Influenza A subtypes
are therefore classified according to the type of HA and NA protein. It
is possible that we do not see such a shift in influenza B because there
is no animal reservoir for this
virus.
Classification of influenza strains:
Type A, B or C/place isolated/number of isolate/year
isolated
In the case of influenza A, also: HA subtype (H) and NA
subtype (N)
There are many flu viruses and they are constantly
changing. The composition of flu vaccines available in the United
States is reviewed annually and updated to match circulating flu
viruses. Flu vaccines protect against the three or four viruses that
research suggests will be most common. For 2016-2017, three-component
vaccines are recommended to contain:
Four component vaccines are recommended to include the
same three viruses above, plus an additional B virus called B/Phuket/3073/2013-like
virus (B/Yamagata lineage).
H1N1 and H3N2 Swine Flu
Swine flu, as its name suggests, is a type A influenza of
pigs and does not normally infect humans. However, swine flu variants do
sometimes spread to humans and in 2009, a new H1N1 swine flu started to circulate. This virus
is unusual because it possesses a combination of genes that have not previously
been observed in animal or human populations. Although the virus is most like
the H1N1 viruses that are found in pigs and was therefore termed "swine flu", it
was found only in humans and did not circulate in pig herds. In response to the
potential for a major pandemic, a mass vaccination campaign using an H1N1 monovalent vaccine (in addition to the usual trivalent vaccine against seasonal
flu) was carried out. In June 2010, WHO declared the pandemic over; however, the
H1N1 "swine" flu continues to circulate around the globe along with the seasonal
flu. It will likely continue to do so. In fact, H1N1 is one of the seasonal flu
strains in the seasonal flu vaccine. Other swine flu variants that have infected
humans include H3N2 and H1N2.
Swine Influenza A H3N2 was first found in the United States in
pigs in 2010 but in recent years a number of human infections have occurred in
people with close contact to pigs. Although the virus can spread directly from
human to human, there has been little spread.
H5N1 Avian Flu
There is concern about a recent outbreak of avian
influenza due to a strain of H5N1 influenza A virus (figure 10B). This bird virus seems to be
able to infect humans without having to undergo a recombination event in some
other animal. The case fatality rate is high (~60%) in humans. Fortunately, as
yet the virus does not readily spread from birds to humans or one human to
another. However, there is concern that it might mutate, or undergo reassortment
with a human influenza virus, and acquire the ability to spread rapidly from
human to human while still being as virulent.
H7N9 Avian Flu
Human infections by this variant have occurred recently in China
and most infections occur in people in close contact with birds. No cases have
been reported outside China.
Although human to human cases have not been reported, the H7N9
virus has genetic changes that may allow it to spread more easily to
mammals, causing more severe disease that spreads rapidly. The case fatality
rate is about 20% and the patients experience a severe respiratory disease that
can lead to pneumonia, acute respiratory distress syndrome and multi-organ
failure.
This variant may have arisen as a result of several
reassortments in which the virus acquired its hemagglutinin from domestic ducks
and its neuraminidase from wild birds with the other genes coming from flu
viruses infecting poultry (Figure 10C).
A
measure of the severity of influenza in any one year is the excess of deaths due
to pneumonia or influenza compared to the seasonally adjusted norm (figure 9).
The World Health Organization (WHO)
maintains constant surveillance of influenza outbreaks world wide and has a
series of 'sentinel' labs to look at what is happening in the circulating virus
population. The CDC does the same
in the United States and co-operates with WHO.
Usually the most important influenza
virus is influenza A, but in some seasons influenza B is the major cause of
influenza. In recent years H1N1 and H3N2 have often co-circulated (figure
10A); the
proportions of each can change dramatically from year to year.
The trivalent inactivated vaccine (TIV) is an
inactivated preparation of egg-grown virus and is given by injection.
The vaccine is reformulated each year according to the strains
circulating around the world.
Only certain formulations of the vaccine are FDA certified for young
children – the annual ACIP recommendations (see below) give details.
Protection is via IgG antibodies.
LIVE, ATTENUATED INFLUENZA VIRUS VACCINE (LAIV)
The live, attenuated influenza virus (LAIV -
marketed as FluMist) vaccine (see
Viral Genetics) is prepared from egg-grown virus. It is approved for
healthy (those not at risk for complications from influenza infection),
non-pregnant individuals 2 to 49 years old but should not be given to
children under 5 years of age who have possible reactive airways disease
(for example, a history of recurrent wheezing). It is given nasally and
should provide mucosal, humoral and cell-mediated immunity. It is
contraindicated for children and adolescents on any therapy containing
aspirin due to the potential risk of Reye's syndrome since the virus is
a live virus.
NOTE FOR 2016 - 2017 FROM CDC
In light of low effectiveness against
influenza A(H1N1)pdm09 in the United States during the 2013–14
and 2015–16 seasons, for the 2016–17 season, ACIP makes the
interim recommendation that LAIV4 should not be used. Because
LAIV4 is still a licensed vaccine that might be available and
that some providers might elect to use, for informational
purposes, reference is made to previous recommendations for its
use.
Both influenza vaccines are formulated annually
using the types and strains of influenza predicted to be the major problems
for that year (the predictions are based on worldwide monitoring of
influenza). The vaccines are multivalent, the current ones are trivalent and
have two strains of influenza A and one of influenza B. Vaccination needs to
be given every year because the most effective strains for the vaccine will
change due to drift and/or shift. The vaccines are usually given in the Fall
(figure 11), once the strains to be used for the influenza season have been
determined in the earlier part of the year. By giving the vaccine in the
fall, protection should be high at the time the influenza season peaks.
Since both vaccines are grown in eggs, they are contraindicated for those
allergic to eggs.
The CDC recommends: "Physicians should administer influenza vaccine to any
person who wishes to reduce the likelihood of becoming ill with influenza
(the vaccine can be administered to children as young as 6 months). Persons
who provide essential community services should be considered for
vaccination to minimize disruption of essential activities during influenza
outbreaks. Students or other persons in institutional settings (e.g., those
who reside in dormitories) should be encouraged to receive vaccine to
minimize the disruption of routine activities during epidemics."
Two neuraminidase inhibitors have been approved by the
FDA (Zanamivir [Relenza] and Oseltamivir [Tamiflu]). They are active against
both influenza A
and influenza B and can reduce the duration of uncomplicated influenza
(by approximately 1day in about 70-90% of adults) if taken within two days of
the onset of illness. However, oseltamivir resistance has been seen in some
circulating strains recently.
To date there are only a few studies of how effective these
drugs are in reducing serious complications in high risk groups when used to
treat influenza (as contrasted with when used prophylactically). Some
limited data suggest they may be beneficial. However, both are approved for prophylaxis as well as treatment.
Rimantadine and amantadine
Rimantadine and amantadine block virus
entry across the endosome and also interfere with virus release (see
Anti-viral
chemotherapy). They may be given as protective agents during an outbreak,
especially to those at severe risk and key personnel.
These drugs were widely used. However, in the 2005-2006
influenza season 92% of the H3N2 strains examined had a mutation which would
confer resistance to these drugs, as did 25% of the H1N1 strains tested -
similar problems have been seen in seasons since then so these drugs are not
recommended until the level of resistance in the major circulating strains
drops. In the absence of the resistant mutations they were good prophylactic
agents for influenza A (but not for influenza B), although there are some
problems in taking them on a long term basis. They could be given to protect
during an outbreak - especially those at severe risk and key personnel. They
could also be given at the time of vaccination for a few weeks - until the
humoral response had time to develop. There is some evidence that
rimantidine and amantadine can reduce the duration of non-resistant
influenza A if given early in infection.
You should check with the CDC MMWR Recommendations and Reports for Influenza for
concerns such as dosage, side effects, and the annual update of recommendations.
The best treatments are rest, liquids, anti-febrile agents (not
aspirin in the young or adolescent, since Reye's syndrome is a potential problem). Be aware of and treat complications
appropriately.
Influenza H5N1 (seen in gold) grown in MDCK cells (seen in
green) CDC/C. Goldsmith, J. Katz, and S. Zaki
COMPARISON
OF INFLUENZA A, B AND C
TYPE A
TYPE
B
TYPE C
Severity of illness
++++
++
+
Animal reservoir
yes
no
no
Human pandemics
yes
no
no
Human epidemics
yes
yes
no (sporadic)
Antigenic changes
shift, drift
drift
drift
Segmented genome
yes
yes
yes
Amantadine, rimantidine
sensitive
no effect
no effect
Zanamivir (Relenza)
sensitive
sensitive
Surface glycoproteins
2
2
(1)
COMPARISON OF
SEASONAL AND PANDEMIC FLU
SEASONAL
PANDEMIC
•Outbreaks follow predictable seasonal patterns;
occurs annually, usually in winter, in temperate
climates
•
•Usually some immunity built up from previous exposure
•
•Healthy adults usually not at risk for serious
complications; the very young, the elderly and
those with certain underlying health conditions
at increased risk for serious complications
•Health systems can usually meet public and patient needs
•Vaccine developed based on known flu strains and available
for annual flu season
•Adequate supplies of anti-virals are usually available
•Average U.S. deaths approximately 36,000/yr
•
•Symptoms: fever, cough, runny nose, muscle pain. Deaths
often caused by complications, such as
pneumonia.
•Generally causes modest impact on society (e.g., some
school closing, encouragement of people who are
sick to stay home)
•
•Manageable impact on domestic and world economy
•
•Occurs rarely (a few times a
century)
•
•
–
•No previous exposure; little or no
pre-existing immunity
•
•Healthy people may be at increased risk
for serious complications
•
»
•Health systems may be overwhelmed
•
•Vaccine probably would not be available
in the early stages of a pandemic
•Effective anti-virals may be in limited
supply
–
•Number of deaths could be quite high
(e.g., U.S. 1918 death toll approximately
675,000)
•Symptoms may be more severe and
complications more frequent
•
•May cause major impact on society (e.g.
widespread restrictions on travel, closings of
schools and businesses, cancellation of large
public gatherings)
•Potential for severe impact on domestic
and world economy


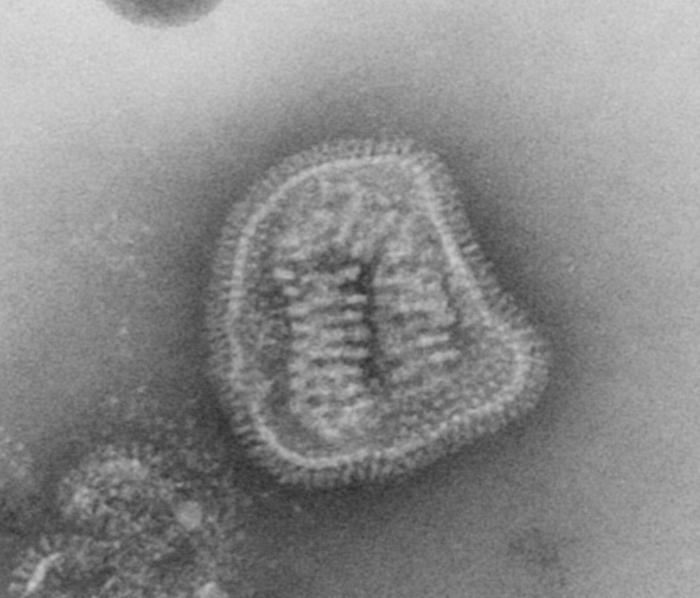
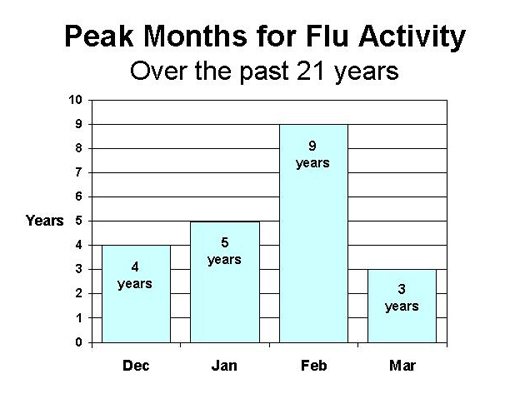 Figure 5
Figure 5 Figure 6A
Figure 6A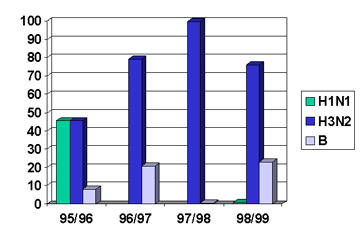 Figure 8
Figure 8 Figure 9
Figure 9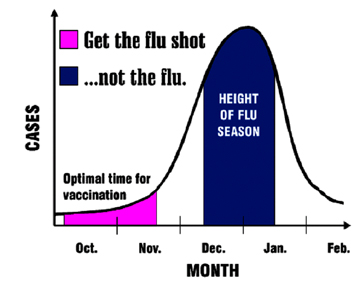 Figure 11
Figure 11 Influenza H5N1 (seen in gold) grown in MDCK cells (seen in
green) CDC/C. Goldsmith, J. Katz, and S. Zaki
Influenza H5N1 (seen in gold) grown in MDCK cells (seen in
green) CDC/C. Goldsmith, J. Katz, and S. Zaki