| x | x | ||||||
|
|
 |
||||||
| INFECTIOUS DISEASE | BACTERIOLOGY | IMMUNOLOGY | MYCOLOGY | PARASITOLOGY | VIROLOGY | ||
|
|
|
||||||
| TURKISH | |||||||
| SHQIP-ALBANIAN | |||||||
|
Let us know what you think FEEDBACK |
|||||||
| SEARCH | |||||||
|
|
|||||||
|
|
|||||||
|
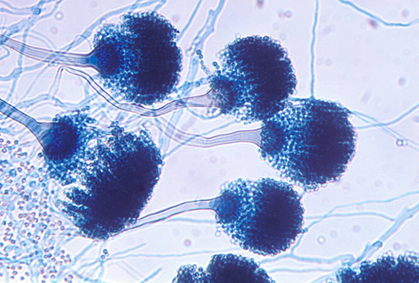
Microscopic morphology of A. fumigatus shows uniseriate conidial heads. Conidiophores are short, smooth-walled, with conical terminal vesicles, supporting a single row of phialides on the upper 2/3 of the vesicle. Conidia are extruded singly from phialides forming chains which usually are disrupted in preparation of slides. Conidia are round and green. Source: #041 (Kaminski library)
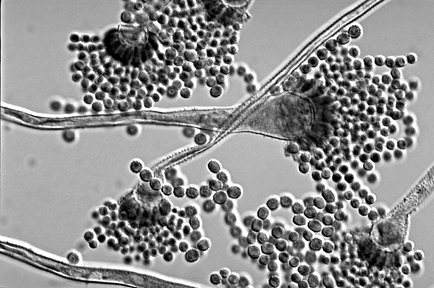
Conidial heads are
biseriate but with some phialides borne directly on the vesicle.
Conidiophores are hyaline and coarsely roughened. Conidia are globose to
subglobose, pale green and spiny.
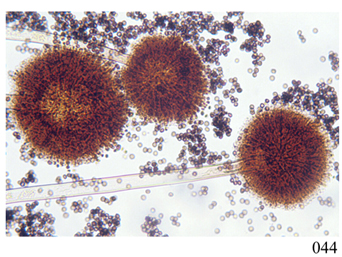
A. niger on Czapek dox agar. Dark-brown to black conidial heads.
|
SYSTEMIC MYCOSES CAUSED BY OPPORTUNISTIC HYALINE MOLDS ASPERGILLOSIS Introduction/Disease Definition Aspergilli produce a wide variety of diseases. Like the mucormycetes, they are ubiquitous in nature and play a significant role in the degradation of plant material as in composting. Similar to Candida species and the mucormycetes they rarely infect immune-normal hosts. These molds are distributed world-wide and are commonly found in soil, food, paint, heat-ventilation-air conditioning systems including those in hospitals. Aspergillosis includes a broad range of clinical forms including:
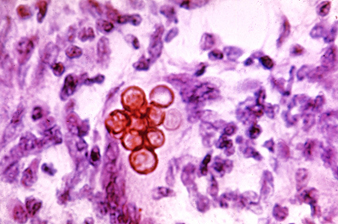
Aspergilli grow as hyaline molds with septate hyphae of uniform diameter that branch at acute angles. Colony colors vary according to the species (see illustrations). The conspicuous microscopic feature is the sporing (conidial) head consisting of a conidiophore terminating in a bulbous vesicle containing one (monoseriate) or two (biseriate) rows of phialides from which round conidia are extruded. The conidia remain attached in columns but are easily dispersed in air currents. In tissue sections Aspergillus hyphae stain poorly with H&E, requiring PAS or GMS for good visibility. Exposure to air spaces in lungs or sinuses may result in formation of conidial heads in situ. Aspergillus hyphae have a predilection for the elastic lamina of blood vessels causing hemorrhage, thrombosis, and infarcts.
Diagnosis The most serious clinical form, IPA, is diagnosed by a combination of radiographic findings and laboratory tests. Diagnostic imaging of pulmonary lesions using CT scan facilitates further testing. Blood cultures are often negative. Sputum cultures and bronchoalveolar lavage fluid are relevant for direct examination and culture. Invasive lung biopsy and histopathology are additional tools. Galactomannan antigenemia in IPA is measured by EIA. Once a culture is growing, morphologic criteria are very useful, and genetic ID may be used if an unusual Aspergillus species is suspected. The specific methods are covered in more detail in the Section: Laboratory Detection, Recovery, and Identification
Etiologic Agents There are more than one hundred species of aspergilli. The most common etiologic agents of aspergillosis in the U.S.A. are:
Geographic Distribution/Ecologic Niche A fumigatus is world-wide in distribution. It is thermotolerant, growing up to 45oC, and is found in composts, wood chips, hay, where it has a role as a cellulose decomposer. A. flavus is a plant pathogen causing post-harvest infestation of corn, peanuts.
Epidemiology, Incidence, and Prevalence Compared with the general population, the incidence of IA and mucormycosis is much higher in patients with hematologic malignancies (HM), hematopoietic stem cell transplants (HSCT), or with solid organ transplants (SOT). Hospital discharge summary data in the U.S. from 2000-2013 for patients with these conditions found a total of169,110 IA cases, for a rate change / million persons over the 13 y period from 32.8 to 46.0, increasing annually by 3% (Vallabhaneni et al., 2017). This increase may be explained by an increased number of HSCT and SOT procedures. With respect to HSCT as a category, a significant decline occurred in the IA rate (-4.6%). Among HM patients the IA the rate did not change significantly. Among SOT recipients, IA rates increased 4.1%. Advances in diagnostics for aspergillosis, (the galactomannan serum assay, chest computed tomography) have increased diagnosis. On the other hand, increased awareness and the use of anti-mold prophylaxis suggest a real decline or stabilization in IA occurred in HSCT and HM patients. Mortality for IA is 20%–50% depending on the underlying condition. But Vallabhanen et al., 2017 found that in-hospital deaths occurred in only 16% of IA (higher in HSCT patients.) Others reported only 40% of invasive fungal infections are diagnosed pre-mortem. There was no difference in fungal disease-free survival with voriconazole when compared with fluconazole among HSCT recipients, but there was a trend toward lower invasive fungal infections, fewer IA infections, and less frequent need for empiric antifungal therapy in the voriconazole arm. This underscores that prophylaxis should be used to prevent IA in HM and HSCT patients during high-risk periods. Prophylaxis may prevent IA but leaves patients susceptible to mucormycosis because of the greater resistance of Mucorales to azoles. Among SOT patients IA increased, with lung transplantation carrying the highest risk.
|
||||||
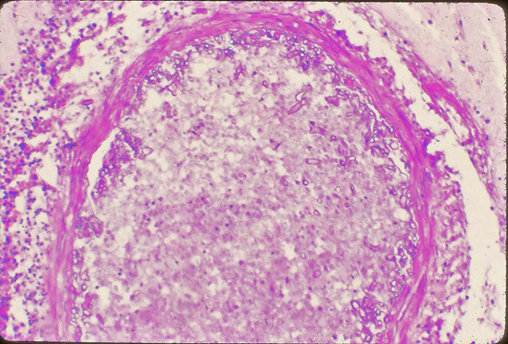
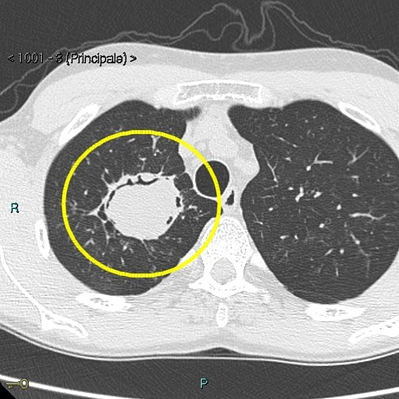 Fig. 4
Fig. 4Aspergilloma (fungus ball) in lung Aspergilloma is a fungus ball that
develops due to the formation of hyphae inside a preexisting lung cavity
(e.g. tuberculosis, sarcoidosis), usually in the upper lobe. CT scan of
lung (axial view) Yellow circle indicates cavity containing fungus ball
and small crescent of air above it. The mycologic term for it is a
mycetoma. |
Summary of Risk Factors for Invasive Aspergillosis Persons receiving cancer chemotherapy, HSCT for hematologic malignancy, other stem cell transplant recipients, patients with solid tumors, or those receiving immunosuppressive therapy for maintenance of SOTs where two of three criteria are satisfied:
Other factors: Defective neutrophil function (e.g.: chronic granulomatous disease), IV drug use, underlying lung disease including tuberculosis.
Transmission Aspergillus conidia, often present in hospital air, are small enough to reach the paranasal sinuses and alveoli. Conidia can circulate through air supply ducts in hospitals and enter chest wounds during surgery. Aspergillosis is not observed in patients housed in laminar air flow rooms.
Determinants of Pathogenicity
Clinical Forms The spectrum of clinical types of pulmonary aspergillosis includes:
|
||||||
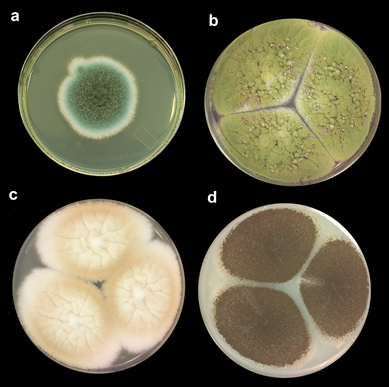 Fig. 5 Colony morphology of major Aspergillus spp.
Fig. 5 Colony morphology of major Aspergillus spp.
a: A. fumigatus
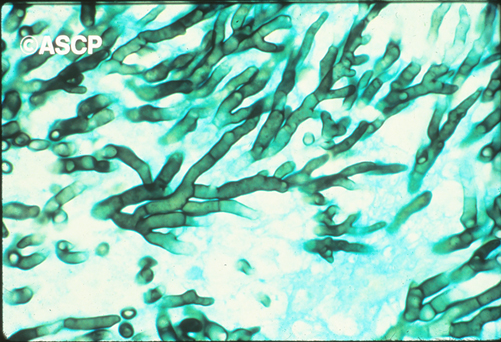
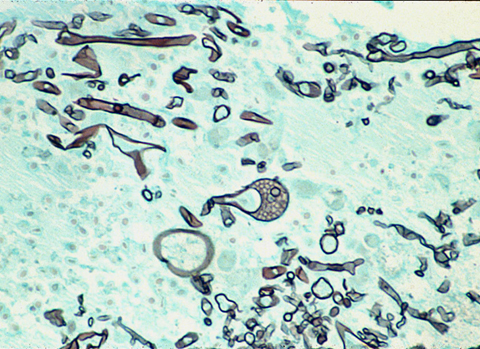
Histopathology—aspergillosis, lung. GMS stain, The septate hyphae are of similar diameter and form acute angle (dichotomous) branching, i.e., a single hypha branches into two even hyphae, and then the mycelium continues branching in this fashion. Reproduced from Chandler FW and JC Watts 1987 Pathologic diagnosis of fungal infections. ASCP Press, Chicago.303 p. with permission from the American Society for Clinical Pathology |
Therapy
Guidelines for diagnosis and management of aspergillosis were updated in 2016 (Patterson et al., 2016). Herein we summarize recommended therapy for invasive aspergillosis. Information about therapy for other forms of aspergillosis are found in that update.
Emerging resistance to azole antifungal agents in strains of Aspergillus fumigatus (Walker et al., 2018). Infections with strains of A. fumigatus resistant to all azole antifungal agents have become common in Western Europe and are emerging in the U.S.A. Pan–azole-resistant A. fumigatus strains with mutations in the cyp51A gene are associated with higher rates of treatment failure and death. These mutations are linked to use of azole fungicides in agricultural and environmental applications and not to prior azole therapy, because patients with these infections frequently lack a history of clinical exposure to azoles. A survey of 1584 U.S. infectious disease physicians was conducted in June 2016. Pan–azole-resistant isolates were reported by 4 (8%) of 51 physicians in the South, 7 (11%) of 63 in the Midwest, 2 (5%) of 37 in the Northeast and 3 (4%) of 70 in the Western U.S. These findings underline the importance of broader susceptibility testing.
Laboratory Detection, Recovery, and Identification
|
||||||
|
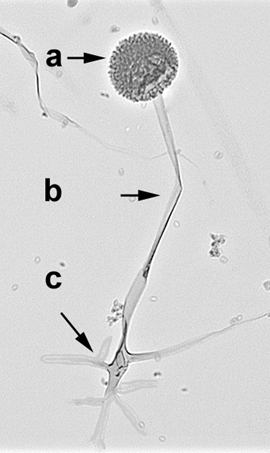
a. Sporangium with sporangiospores b. sporangiophore c. rhizoids. Source: E. Reiss
Mature sporangium of Apophysomyces elegans with the distinctive funnel shaped apophysis. Colonies are fast growing, white, becoming brownish with age, composed of broad, pauci-septate hyphae. Sporangiophores are unbranched tapering towards the apophysis. Sporangiophores are at right angles from the aerial hyphae, anchored by rhizoids. Sporangia are small and pear-shaped. Columellae are rounded and the apophyses are funnel or bell-shaped. Sporangiospores are brown colored in mass. Good growth at 26C, 37C and 42C. Source: #565. Geraldine Kaminski Library of Medical Mycology.
|
MUCORMYCOSIS Disease Definition Mucormycosis* is an acute inflammation of soft tissue, usually with fungal invasion of the blood vessels (angioinvasion) which can rapidly progress to fatal disease in susceptible human hosts. Mucormycosis is caused by several species in the order Mucorales, subphylum Mucoromycotina, (e.g.: Rhizopus oryzae, Lichtheimia (formerly Absidia), Rhizomucor). Mucormycetes are ubiquitous in the environment and rarely cause disease in an immune-normal host. Rhinocerebral mucormycosis can occur in patients with diabetic ketoacidosis. Other underlying conditions which cause susceptibility are: hematologic malignancy, complications of organ or stem cell transplants, severe burns, or intravenous drug use. Post-traumatic mucormycosis (traffic accidents, natural disasters) is another clinical form. (*formerly zygomycosis)
Diagnosis Direct microscopic examination of tissue scrapings, sinus aspirates, bronchoalveolar lavage fluid, biopsy of necrotic tissue, accompanied by culture (these are rapid growing molds.) There are no available serologic tests. Detection of Mucorales DNA in blood is an emerging technology. See “Laboratory Detection…”.
Etiologic Agents The common genera and species causing mucormycosis are (alphabetic order not in order of prevalence: Lichtheimia, Mucor circinelloides, Mucor spp. Rhizomucor, Rhizopus oryzae (Fig. 8). Notable outbreaks of post traumatic mucormycosis have been caused by Apophysomyces. (Fig. 9) See “Epidemiologic Highlight”
Geographic Distribution/Ecologic Niche These fungi are found world-wide, commonly in soil, food, organic debris etc. They are seen on decaying fruit and vegetables in the refrigerator and on moldy bread. Their spores become airborne and may be inhaled, alight on open wounds, or are ingested with contaminated fruit or bread.
Transmission
Sporangiospores of Mucorales are carried on air currents and
inhaled from the environment, or alight on open wounds and burns. As
frequent saprobes on fruit and bread, the sporangiospores may also be
ingested. Determinants of Pathogenicity
Pathogenic factors include iron utilization at acidic pH, and
production of lipase. Bacterial endosymbionts of Rhizopus species
produce toxins implicated in pathogenesis. Further information is
provided in Reiss et al., 2011. Clinical Forms
|
||||||
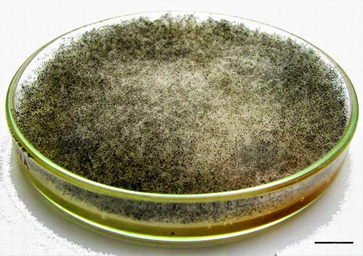 Fig.10.
Fig.10. Pin molds, growth on agar plate Rhizopus stolonifer Source:
Microbiology and our life, Google +https://plus.google.com/
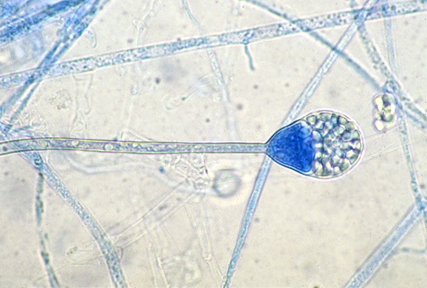
Typical mucormycete hyphae in tissue also shows a sporangium of Lichtheimia species. Source Geraldine Kaminski Library of Medical Mycology #590 |
Therapy Success in mucormycosis requires a combination of: early diagnosis, restoration of euglycemia, reversal of other risk factors, including immunosuppression (if possible), prompt start of antifungal therapy, and surgical debridement (as needed). Delay in using an amphotericin-B based drug (>6 d after diagnosis) may double mortality at 12 wks in patients with diabetes (of all types) (Sun and Singh 2011). Mortality in the 1990’s declined from previous levels to 40%, but outcomes are poor, especially in stem cell transplant patients with disseminated disease where mortality remains in the 90-95% range (Sun and Singh 2011). AmB based agents are preferred for mucormycosis. All-cause mortality varies from 39% to 75% in patients receiving lipid formulations of AmB as primary or salvage therapy. Liposomal AmB delivers improved response and survival compared with AmB deoxycholate. Echinocandins may have a role as combination therapy with AmB. Posaconazole is the first azole with broad activity against Mucorales. Monotherapy with posaconazole is not recommended, instead it is used as salvage therapy. Isavuconazole is a newer triazole approved in the U.S. for treatment of mucormycosis, and when AmB is not feasible. Recently, studies reported cases of breakthrough mucormycosis and other invasive fungal infection in patients receiving isavuconazole as prophylaxis or treatment (Sipsas et al, 2018).
Laboratory Detection, Recovery, and Identification
|
||||||
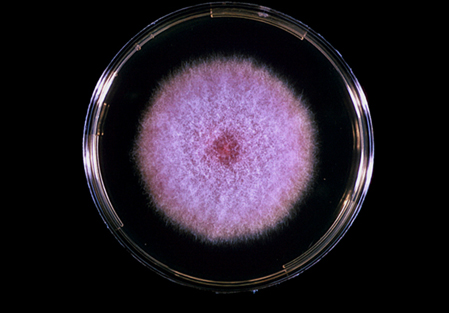 Fig. 12 Colony morphology Fusarium species on Sabouraud dextrose
agar
Fig. 12 Colony morphology Fusarium species on Sabouraud dextrose
agar
Species of Fusarium typically produce both macro- and microconidia. Macroconidia are formed after 4-7 days from short multi-branched conidiophores, They are 3- to 5- septate (usually 3- septate), fusiform, cylindrical, often moderately curved. Source: Geraldine Kaminski library of mycology # 468
In F. solani, microconidia are usually abundant, cylindrical to oval, 1- to 2-celled and formed from long lateral phialides Source: Geraldine Kaminski library of mycology # 467
|
FUSARIUM MYCOSIS Introduction/Disease Definition This is a large genus of plant pathogens also causing disease in humans especially in Immuncompromised patients. Clinical forms include paronychia, sinusitis, pulmonary, and extra-pulmonary disseminated infections. In immune normal patients: locally invasive disease-- mycotic keratitis (at risk are contact lens wearers) and endophthalmitis, onychomycosis, burn infections, sepsis in peritoneal dialysis patients. Etiologic Agents Major pathogens are Fusarium solani and F. oxysporum. Each existing as a species complex.
Geographic Distribution/Ecologic Niche World-wide, all climatic zones in soil, plant debris, on plants. Dispersal of conidia occurs in air and in water (including hospital water supply, especially F. oxysporum.
Incidence Fusarium species are the most frequent mold cause of mycotic keratitis and are second to Aspergillus as cause of invasive mycosis in stem cell transplant (SCT) patients. Rates vary widely among institutions.
Risk Groups/Factors
Transmission Inhaled conidia including aerosols from hospital water supply or other water source; ingestion or injection through skin trauma.
Produce mycotoxins but their role in disease is unknown. Angioinvasive tendency leading to thrombosis, infarcts.
Clinical Forms
Therapy Invasive treatment of Fusarium keratitis and endophthalmitis is frequently necessary. Outcome can be poor including the possibility of enucleations. Long delays before the correct diagnosis is a risk factor for poor outcome. Steroid use which suppresses inflammation may also contribute to delayed diagnosis due to intraocular spread. Amphotericin B has the lowest MICs for Fusarium spp. MICs for another polyene, natamycin, are higher but isolates with MICs of <16 µg/mL are considered susceptible to natamycin, because those concentrations are reached in the eye. Natamycin, due to its smaller molecular size, may more easily penetrate the eye than AmB. Resistance to most antifungals is typical of Fusarium species which are innately resistant to echinocandins, and have high MICs with respect to azoles. All isolates of the FSSC had MICs for terbinafine of >32 µg/mL, whereas other Fusarium species had terbinafine MICs of < 8 µg/mL.
Risk factors
Therapy Deep-seated Fusarium spp. infections are refractory to treatment. The drug of choice for the treatment of invasive fusariosis is either voriconazole or liposomal amphotericin B. The outcome is usually poor, and largely dependent on the recovery of the immune status of the host, particularly from neutropenia. Natamycin drops for keratitis; nystatin cream for skin lesions.
Laboratory Detection, Recovery, and Identification Skin lesions and blood cultures are the main specimens for diagnosis. Biopsy of skin lesions for histopathology and culture; Histopathology reveals branching hyaline, septate hyphae, invading blood vessels. In contrast to aspergillosis, blood cultures are frequently positive. KOH preparations from nail clippings, skin scrapings, corneal specimens in cases of keratitis are useful.
|
||||||
|
Microscopic morphology of Scedosprium apiospermum shows numerous, single-celled, pale-brown, broadly clavate to ovoid conidia, borne singly or in small groups on elongate, simple or branched conidiophores or laterally on hyphae. Source: Geraldine Kaminski library of mycology 525. |
PSEUDALLESCHERIA/SCEDOSPORIUM MYCOSIS
Introduction/ Disease Definition Subcutaneous, sino-pulmonary, and pulmonary-disseminated infections caused by the molds in the Pseudallescheria boydii species complex and other Scedosporium species. Portal of entry is either respiratory via inhalation of conidia or by traumatic implantation of thorny plants and splinters. Eumycetoma is a special category of subcutaneous mycosis and is discussed separately
Specimens including biopsy
material, BAL fluid, bronchial washings, CSF, sputum, tracheal aspirates are
examined in 10% KOH preps. Detection is improved with Calcofluor
fluorescent brightener. Gram-stained smears show acute angle branched, septate
hyaline hyphae similar to that of other hyaline molds, but may show an irregular
branching pattern. Etiologic Agents Environmental molds: Pseudallescheria boydii; Scedosporium apiospermum and minor species. Scedosporium prolificans reclassed as Lomentospora prolificans is a melanized mold.
Geographic Distribution/Ecologic Niche Worldwide agents of sino-pulmonary and pulmonary- disseminated mycosis in immunocompromised hosts. Causes eumycetoma in N America. These species are isolated from agricultural soil, sewage, and polluted water.
Epidemiology An emerging mycosis in immunocompromised hosts, third in prevalence behind aspergillosis and Fusarium mycosis. Approximately 1%-27% (depending on study design) of opportunistic mold mycoses are caused by non-Aspergillus species molds.
Risk Groups/Factors Immune-normal host: occupational or recreational exposure to penetrating injuries, contact lens wearers, near-drowning accident victims, cystic fibrosis patients. Immunocompromised host: Patients with hematologic malignancy, stem cell- and organ transplant recipients.
Transmission Traumatic implantation or inhalation of conidia, aspiration of conidia in water (near drowning accidents).
Determinants of Pathogenicity
Clinical Forms
Fungal sinusitis, pneumonia, fungus ball
in a preexisting pulmonary cavity, extrapulmonary dissemination, cerebral
abscess. May be neurotropic with the CNS as a site of dissemination.
Also a cause of
Eumycetoma (See EUMYCETOMA sub-section, below) Therapy
Pseudallescheria/Scedosporium
species are less susceptible to AmB
than Aspergillus fumigatus; voriconazole (VRC) is the preferred therapy;
L. prolificans is refractory to most monotherapy, may be responsive to
combination therapy. Laboratory Detection, Recovery, and Identification Specimens for direct examination and culture: grains, skin scrapings, exudates, sputum, sinus drainage, invasive biopsy including drainage from closed cerebral abscess; blood cultures. Growth is rapid on SDA. May demonstrate sexual reproduction: cleistothecia with ascospores after 2-3 weeks incubation, or after transfer to cornmeal agar. Asexual reproduction is enteroblastic with single large obovoid annelloconidia (Fig. 14). Sometimes conidiophores are in small clusters: synnemata. Histopathology: difficult to distinguish from Aspergillus species. Sometimes chlamydospores and conidia are produced in vivo; L. prolificans gives a positive Fontana-Masson staining reaction in tissue for melanin. |
||||||
|
Microscopic morphology of Cladophialophora carrionii (magnified 475X). Elongate conidiophores produce branched acropetal chains of smooth-walled conidia. A common cause of chromoblastomycosis particularly prevalent in arid and semi-arid areas, most often in tropical and subtropical zones. Source: CDC/Dr. Lucille K. Georg
Conidia-laden conidiophores of a Phialophora verrucosa from a slide culture. Flask-shaped phialides, each lipped by a collarette. Each phialide terminates in a bundle of round, to ovoid conidia. Phialophora spp. are causative agents of both chromoblastomycosis, and phaeohyphomycosis. Source: CDC/Dr. Libero Ajello
|
MYCOSES OF IMPLANTATION CAUSED BY MELANIZED MOLDS
CHROMOBLASTOMYCOSIS
Introduction/Disease Definition This is a chronic, localized infection of subcutaneous tissues caused by several species of melanized fungi. The route of entry is usually by penetrating injury with a thorn or splinter containing the fungal elements resulting in lesions most often on the arm, foot or leg. Most aspects of this disease are reviewed in Queiroz-Telles et al., 2017.
Diagnosis Physical diagnosis depends on the presence of chronic cutaneous and subcutaneous nodules or plaques that enlarge over time to become verrucous (Fig. 15). Laboratory diagnosis is facilitated by histopathology and culture. The tissue form is unique and diagnostic, consisting of a cluster of round, thick-walled cells that divide by internal cleavage planes (def: sclerotic bodies, or muriform cells) (Fig. 16). They appear in H&E stained tissue as brown or copper-colored, the so-called “copper pennies”. These cells occur in tissue of most if not all agents of chromoblastomycosis. Speciation is determined by the pattern of conidiogenesis of the mold form in slide cultures on SDA agar.
Etiologic Agents The etiologic agents of chromoblastomycosis are septate, slow growing molds, darkly pigmented members of a single family the Herpotrichiellaceae. The most common agents are:
Exophiala spp. are occasional causes of chromoblastomycosis but most often cause other infections. This genus produces a mucoid yeast form, but as the culture ages the mucoid appearance dries and becomes more hyphal.
Geographic Distribution/Ecologic Niche
The causative agents
are
saprobes located in soil and decaying vegetation, world-wide.
Epidemiology
Barefoot
labor in tropical or subtropical areas. Transmission
There is no known
person-to-person transmission. Clinical Forms
These fungi induce a granulomatous reaction:
pseudoepitheliomatous hyperplasia. The lesions, growing slowly over mo
or years become cauliflower-like, with the affected limb becoming
distorted by fibrosis and lymphedema (Fig. 15) Therapy Small early lesions can be removed surgically. Lesions in moderate to severe clinical forms are refractory and healing is very difficult, requiring long-term systemic antifungal treatment. The following methods are used in addition to antifungal agents:
Laboratory
Detection, Recovery, and Identification
Direct
examination. Surface scrapings from the surface of warty lesions
mounted in 10% KOH preps may reveal round brown sclerotic bodies (muriform
cells) dividing by transverse septations.
Histopathology. Biopsy of skin lesions stained with H&E will also
show the characteristic sclerotic bodies (Fig. 18).
Culture.
Crust, exudates, part of minced biopsy specimens planted on SDA with
antibiotics and cycloheximide. Small dark green to black colonies
become evident after 10 d to 2 wks. Species identification is
determined by slide culture on PDA.
In Vitro Antifungal Susceptibility Itraconazole, posaconazole, voriconazole and isavuconazole show the best in vitro activity against agents of chromoblastomycosis, but amphotericin B, 5-fluorcytosine, fluconazole and echinocandins have limited activity.
First-Line Therapy Itraconazole is standard therapy for chromoblastomycosis with cure rates ranging from 15-to 80%. An oral capsule form shows clinically significant activity against most chromoblastomycosis agents being more effective against C. carrionii than against F. pedrosoi. Clinical and mycologic cure can be achieved with long term therapy for many mo. When lesion reduction has occurred cryosurgery can be applied to remove the remaining lesions. Terbinafine is the second most frequently used antifungal agent for chromoblastomycosis with cure rates after long-term therapy similar to those achieved with itraconazole. Terbinafine has fewer drug interactions than itraconazole and may also possess an antifibrotic effect. Combination therapy, usually with itraconazole and terbinafine, has been used as the last option salvage therapy for refractory or advanced chromoblastomycosis or when monotherapy has failed. In vitro studies have not shown synergism or antagonism of this combination. Among extended-spectrum triazoles, posaconazole has the best potential for treating chromoblastomycosis, including severe or refractory forms. Posaconazole has broad in vitro activity against most melanized fungi including causative agents of chromoblastomycosis and phaeohyphomycosis. In addition to oral suspensions are newer delayed released tablets. Delayed-release posaconazole tablets may achieve higher average plasma concentrations than those achieved with the oral solution and are well-tolerated. Posaconazole oral solution has better pharmacodynamic and pharmacokinetic profiles than the itraconazole capsule formulation. Oral voriconazole has been used to good effect in a few cases of refractory disease. Isavuconazole is very effective in vitro against melanized fungi, and is another therapeutic option.
|
||||||
 Fig. 19. Microscopic morphology Exserohilum rostratum
Fig. 19. Microscopic morphology Exserohilum rostratum
See text for description. Photo credit: Hernández-Restrepo M, et al., 2018 (open access creative commons license) |
PHAEOHYPHOMYCOSIS (Phaeo def: (Gr.: dark)
Phaeohyphomycosis includes 3 different clinical forms: – Cutaneous-subcutaneous cysts: lesions are cystic, nodular, verrucous, ulcerated, or plaque types – Cerebral abscess and other deep-seated sites of infection – Fungal sinusitis The disease is defined by the appearance of fungi in tissue (a histopathologic definition): – It includes melanized molds and yeastlike relatives which grow in tissue or in the nasal sinuses as hyphae, or a mix of hyphae and yeast forms.
Clinical Forms and their Etiologic agents
Therapy
About Exserohilum rostratum Exserohilum is a melanized mold classed in the Pleosporaceae, Pleosporales in a well-supported clade separate from related Curvularia and Bipolaris spp. Exserohilum may infect immunocompromised and immune-normal hosts with clinical forms ranging from cutaneous infections (phaeohyphomycosis) to disseminated disease, also including allergic fungal sinusitis. E. rostratum is a plant pathogen affecting a range of species particularly grasses. Growth is rapid on PDA plates (sporulation more intense on 15% V-8 juice agar.) E. rostratum grows on medium containing benomyl, 10 µg/mL.
|
||||||
 Fig. 20
Fig. 20Foot eumycetoma A massive foot eumycetoma with multiple sinuses and
discharge with black grains. |
EUMYCETOMA Mycetomas are localized chronic granulomatous infections of the cutaneous and subcutaneous tissues, usually on the lower extremities (less commonly on the hand, chest or back). Infection initiates after a penetrating injury from plant material, a thorn or splinter, containing the fungus. Slowly, over months and years, multiple granulomas and abscesses develop containing large aggregates of fungal hyphae (Fig. 20). (Fahal et al., 2015) Fistulas
form with draining sinus tracts discharging grains, which are compact
masses of fungal hyphae embedded in a cement-like extracellular matrix.
Fibrosis around the grains is often severe. Tumefaction (indurated
swelling) of the limb ensues. Eventually the affected limb is deformed
with destruction of muscle, fascia, and bone (osteomyelitis).
Hematogenous or lymphatic spread from a primary focus to distant sites
is very rare. Synonyms: Madura foot, anthill foot (arch.).
Eumycetoma is caused by a variety of true fungi, whereas bacterial
mycetoma is caused by actinomycetes. Diagnosis
of the etiologic agent, whether eumycetoma or actinomycetoma, is
essential for patient management because the prognosis and therapy
differs. Geographic distribution Eumycetoma is endemic in the tropics and subtropics between latitudes 15°S and 30°N around the Tropic of Cancer (23.5oN). The major endemic area is in Sudan; other areas are Mexico, Central and S America, India, Indonesia, Pakistan, other African countries, the Middle East, occasionally in temperate zones including the U.S.A.
Etiologic agents The number of fungi producing eumycetoma is upwards of 21-30 species; both hyaline and melanized molds may be involved. Madurella mycetomatis, occurring in the arid regions of Africa, accounts for most cases worldwide, causing > 70% of cases in Central Africa including the Sudan. Madurella grisea is a common etiologic agent in S America. Leptosphaeria senegalensis and Leptosphaeria tompkinsii are common causes in W Africa. Pseudallescheria boydii and Scedosporium spp. are the most common causes in U.S.A. Major agents of actinomycotic mycetoma are Nocardia brasiliensis, Actinomadura madurae, Streptomyces somaliensis,
Therapy Surgery and long-term oral azole and/or terbinafine therapy. Most patients with eumycetoma are treated with either ketoconazole or itraconazole (Welsh et al., 2014). Itraconazole 200–400 mg/d for 6 mo is used to create a fibrous capsule around the lesion, followed by wide local excision, continuing itraconazole, 200–400 mg/d, until cure is achieved. Cure is defined as disappearance of the mass, all sinuses, normal ultrasound, and negative mycology. The decision to stop therapy is determined by complete sinus healing, disappearance of the eumycetoma mass clinically and radiologically by CT scan or MRI, and absence of the infecting agent. Other antifungal agents used as second-line treatment include voriconazole and posaconazole.
Laboratory Detection is by examination of grains, biopsies, curettage from sinuses, and culture, molecular identification: PCR of rDNA. Grains are seen in a variety of colors (white, brown, yellow, black)
The three most common etiologic agents are:
*The most common in the US. These organisms are associated with the soil, thus you see many infections in the feet and legs. Clinical specimens for diagnosis: are pus containing grains, white, yellow, brown, or black; and tissue for histology. The color, size and texture of the grains aid in the diagnosis of mycetomas. Eumycotic mycetoma grains are visible to the unaided eye and measure 0.2 mm to several mm diam and contain hyphae 2-6 µm or larger in diam. Grains containing actinomycetes, have bacterial elements <2 µm diam. Washed grains mounted in 10%KOH are examined microscopically for size of filaments, color.
Culture The agents of eumycetoma are all filamentous fungi which require at least 7-10 days for visible growth on the culture media and then another several days for specific identification. These fungi are identified by their colonial morphology, conidia formation, and biochemical reactions. Medium for fungal growth is Emmons’ modified Sabouraud dextrose agar containing antibiotics but not cycloheximide. Cultures are held for 6-8 wks.
Histopathology H&E is a good first choice stain because microscopic structure of grains is readily visible. Gomori methenamine silver (GMS) or PAS stain is applied for eumycetoma grains, whereas Brown and Brenn stain is used for actinomycotic mycetoma. The species of fungi cannot be distinguished in histopathologic tissue sections. Fungi appear as branched septate hyphae, often distorted in shape and with chlamydospores at the periphery of grains. Images of histopathologic sections may be found in Chandler et al., 1980.
|
||||||
|
|||||||